

Key takeaways
A document presented at the 2026 CCMG/Garrod conference connects phenylketonuria to a broader burden than blood Phe alone: comorbidities, restriction of natural protein, and quality of life.
As we age with PKU, the question is not only how to control a blood test result, but how to preserve overall health.
Sephience does not solve everything, but if it allows some people to lower their Phe and increase natural protein intake, it could reduce an important part of the long-term burden.
Disclaimer: I am not a physician. This text reflects my personal experience with phenylketonuria and my reading of the available data. It does not replace advice from a metabolic team. Any change to treatment, diet, or natural protein intake should be made with a healthcare professional.
When we talk about phenylketonuria, we almost always come back to the same number: the level of phenylalanine (Phe) in the blood. That makes sense. Phe is at the center of the disease. It guides decisions, dietary adjustments, treatments, and even the mental state of the week. But the older I get, the more I wonder whether this number, as important as it is, only tells part of the story.
A document presented at the 2026 joint conference of the Canadian College of Medical Geneticists and Garrod struck me for that reason. It does not speak only about Phe as a laboratory result. It tries to connect several dimensions of PKU: elevated phenylalanine levels, neurocognitive symptoms, comorbidities, chronic restriction of natural protein, and quality of life. The document comes from PTC Therapeutics, so it should be read with the necessary caution when a pharmaceutical company produces a review in its own field. But the question it raises matters: what does a whole life with PKU do?
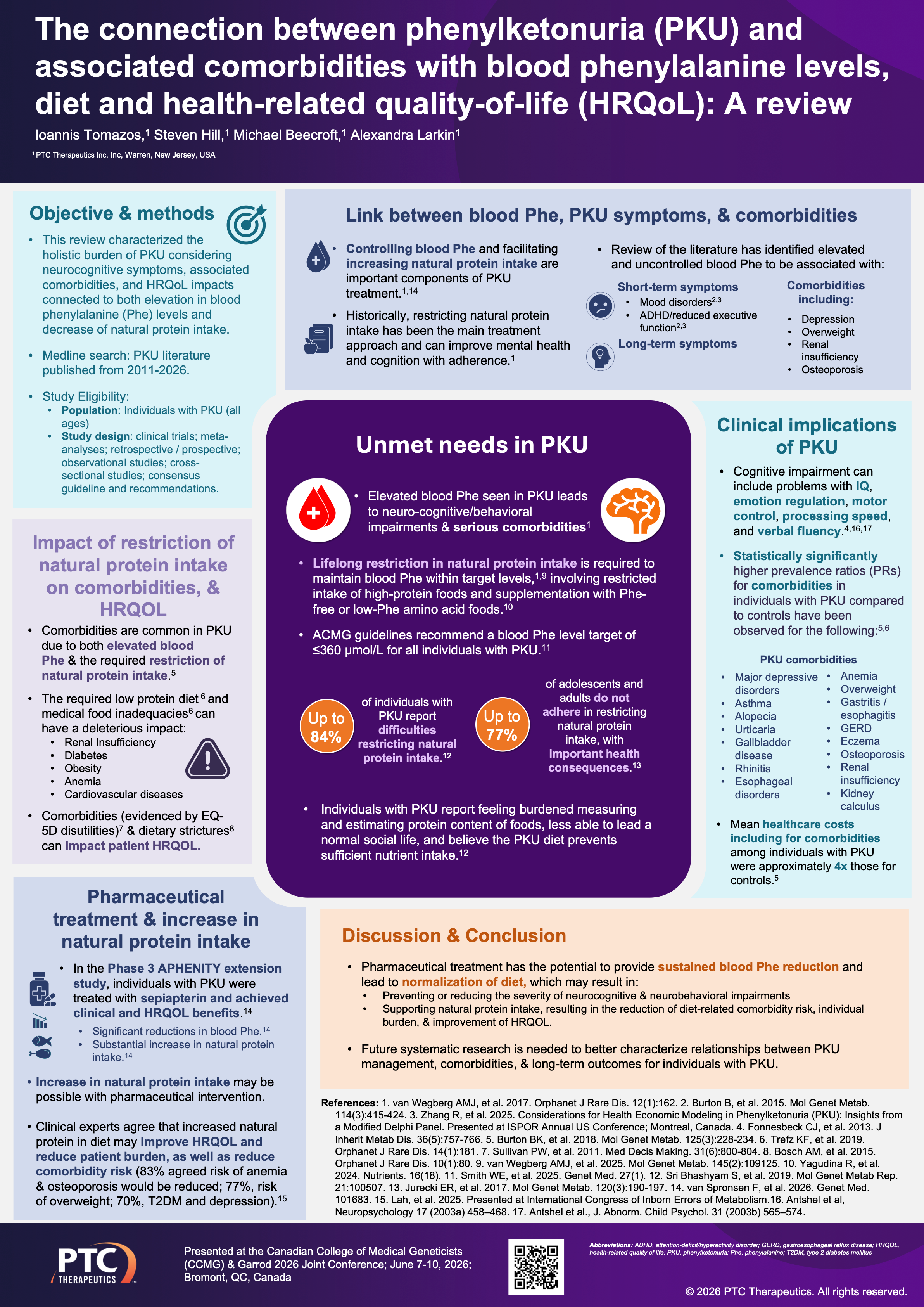
The document, one of many reviewed and accepted at this medical/scientific meeting, reminds us that comorbidities are common in PKU and may be connected to two realities that move together: on one side, Phe levels that are too high; on the other, the restriction of natural protein required to control them. It mentions issues such as anemia, overweight, obesity, osteoporosis, renal insufficiency, kidney stones, some digestive disorders, cardiovascular disease, diabetes, mood disorders, and cognitive or executive-function difficulties. This list should not be read as an individual sentence. These are not certainties for every person. But they are signals that force us to look at PKU as a lifelong condition, along with other conditions affecting many, not only as a Phe problem to manage meal by meal.
I do not read this in an abstract way. I read it as someone who lives with PKU, who has a daughter (without PKU), who has worked very hard to build a good life, and who wants to stay here for a long time. I want to be able to play and talk with my daughter and run with my grandchildren. I would like to age in good health, keep my mind, my independence, my energy, and my ability to be present. But when you live with a metabolic disease from birth, you need to think beyond the next blood test. And right now, no one really knows what will happen to PKU patients with elevated Phe levels when they reach 80 years old or older.
This is where comorbidities become very concrete. Obesity, insulin resistance, inflammation, metabolic problems, age-related muscle loss: these are not topics separate from PKU. They are part of the same body. A person with PKU can also age, gain weight, lose muscle, sleep less well, become more metabolically vulnerable, or see their cognitive health become more fragile. PKU does not explain everything, and we should not attribute every health problem to it. But it would be too simple to say that a whole life of dietary restriction, sometimes elevated Phe, and dependence on specialized products has no effect on overall health.
Sarcopenia, for example, is not at the center of the document, but it is at the center of my concerns. As we age, losing muscle is not about appearance. It is about losing reserve. It means having more difficulty walking, recovering, staying independent, getting through an illness or a harder period. In the general population, there is more and more discussion about the importance of protein, resistance training, and maintaining muscle mass with age. In PKU, that discussion is more complicated, because natural, muscle-building protein is precisely what we restrict.
Protein substitutes are essential. They have allowed generations of people with PKU to develop, function, work, and live a life. But in real life, it is not the same thing as a freer, more varied, more normal diet with normal nutrition. It is not only a question of nutrition on paper. It is also a question of satiety, pleasure, simplicity, mental fatigue, and one’s relationship with food. Many people with PKU know the feeling of always having to compensate, always plan, always explain, sometimes always be hungry, or never quite eat like everyone else. This constant management has heavy social and cognitive impacts.
This is the context in which Sephience becomes interesting to me. Not as a miracle solution. Not as a promise that everything disappears. Not as a medication that replaces medical follow-up. But as a possibility to reduce the burden in two places at once: Phe and dietary restriction.
I have already written about the comparison between Sephience and Kuvan in my previous article on the burden of the low-phenylalanine diet. The essential point remains the same: the AMPLIPHY study directly compares sepiapterin, the active ingredient in Sephience, with sapropterin, known as Kuvan. In people who responded to sepiapterin, Sephience reduced Phe more than the maximum approved dose of sapropterin. This matters because Kuvan has helped some people, but it has never transformed life for everyone. For many people with PKU, diet has remained at the center of treatment, with all the burden that comes with it.
But for me, the most important question comes after the Phe reduction: what can a better reduction in Phe make possible in real life? This is where the APHENITY extension data become relevant. In that study, some people treated with sepiapterin were able to significantly increase their dietary Phe intake, meaning natural protein, while being monitored. The nuance matters. Sephience does not mean abandoning the diet. The Canadian Sephience product monograph states that the treatment should be used with a phenylalanine-restricted diet, as recommended by a healthcare professional, and that response must be assessed individually.
But increasing natural protein in PKU is not a minor comfort detail. It is potentially a life less organized around the disease. Fewer calculations. Fewer specialized products. Fewer separate meals. Less mental load. Maybe better satiety. Maybe a diet that is denser, simpler, and more sustainable. And over time, that margin can become important.
The conference document does not prove that Sephience will prevent obesity, insulin resistance, osteoporosis, kidney problems, or sarcopenia. That would go too far. Rather, it shows that PKU needs to be considered more globally. It shows that comorbidities exist, that the dietary burden is real, that quality of life is affected, and that restricting natural protein for a lifetime is not simply a medical strategy without consequences. That is already a lot.
I think this is where the discussion around Sephience should be situated. Not only in a logic of a medication that is more effective than Kuvan. Not only in a short-term pricing logic. And not in an overly quick promise of cognitive or physical improvement either. We should instead ask what better metabolic control and greater natural protein tolerance could change in our overall wellbeing over several years.
PKU often forces us to think in days:
How much Phe today?
What blood result this week?
How much natural protein in this meal?
But aging with PKU forces us to think in decades:
What cognitive health at 70?
What strength at 80?
What independence?
What metabolic risk?
What economic burden for the healthcare system?
What quality of life for families?
What ability to remain present for the people we love?
That is probably what touches me most in these data. They remind me that I do not only want to survive with PKU. I want to age with as much capability and reserve as possible. Cognitive reserve, muscle reserve, metabolic reserve, emotional reserve. I want to keep my place in my family. I want to be there for my daughter. I want, if I get that chance, to be a present, healthy, and fit grandfather.
Sephience does not guarantee that. No treatment can guarantee that. But if it allows some people to better control their Phe while increasing natural protein intake, then its importance is not limited to a better value in a table. It could help make life with PKU a little less organized around restriction, and a little more oriented toward long-term health.
And for me, that is where the subject becomes truly human. The question is not only whether Sephience is impressive. The question is whether it can give more margin to people who have lived with PKU from the beginning. More margin to eat. More margin to think. More margin to age. More margin to live.
As a nurse, it's been my experience that people in general tend to overestimate how long they will live. Here in the U.S. average lifespan for women is about 80 and for men 76. That means midlife for women is around 40 and for men 38. People don't tend to feel "older" when they're in their 30s and 40s though! However, in the hospital I take care of people in their 50s and 60s every day who are experiencing life- altering disease and disability. In fact, most people in this country don't make it all the way to retirement age of 65, and the leading cause of early retirement is medical issues. (I always tell people, if you want to do something don't wait...just go for it!) That's an overall view of the general population, but people living with a chronic illness tend to have reduced lifespan. Elevated phe levels over a lifetime have a cumulative negative effect, unfortunately. Here in NY we started testing for PKU in 1965, so that would mean if they stayed continously on treatment, our oldest PKU patients would be coming into their 60s now. There isn't any tracking or comprehensive data on these patients though, so we don't know how they are faring health-wise. We also don't know if they are able to access meds like Kuvan or Saphience. I have been appealing to my insurance for over a year now and so far have not been able to trial either drug, and I have good insurance. Saphience appears to have an additional method of action that Kuvan lacks, and so I hope it will become more widely available in the future.
Thank you for your insight and dedication. Sephience did not work for me so I went back to my LNAA that I have been in for 20 odd years. This allows me more protein per day and gives me the benefits you talk about, but still, pkuer’ers in old age and the effects of diet, levels and medicines ( formulas and pharmaceuticals) still remains a mystery for healthcare workers and patients alike. I guided my dad through a diet for kidney disease ( since I understood nutrition better than him) and saw how incompatible the pku diet is with the kidney diet. So yes, there is a lot of work to be done still- just in terms of co-morbidities that can be more harmful than pku itself. I appriciate your writings and discussion of these because being an “older pku’er” is often left aside.